

Key Points
- One of the important functions of the cruciate ligament is to prevent backward sliding of the femur on the tibia bone, also known as drawer motion
- Rupture of this ligament leads to debilitating lameness
- The TPLO surgery compared to other techniques results in
+ a more rapid recovery
+ better range of motion of the joint
+ development of less arthritis
+ return to athletic or working activity
- Most dogs have a very good outcome with TPLO surgery
Downloadable forms/information for clients for initial visit:
Client initial consultation history sheet
Discharge instructions for TPLO postop care
Downloadable forms/information for clients for recheck visits:
2-week TPLO discharge instructions
8-week TPLO recheck (in hospital)
8-week TPLO discharge instructions
Downloadable forms for referring veterinarians:
Below is a video that summarizes the highlights of the TPLO surgery in dogs
Introduction
The stifle joint of the dog is equivalent to a human’s knee. The cranial cruciate ligament is located inside the joint and is responsible for maintaining a stable joint. One of the important functions of the ligament is to prevent backward sliding of the femur on the top of the tibia bone (called drawer motion). Cranial cruciate ligament rupture is the most common orthopedic condition that we treat at ASCM. This problem afflicts all ages and breeds of dogs. Cruciate ligament rupture is usually a progressive process and not due to a single traumatic injury. Most dogs have predisposing factors such as age-related ligament degeneration, pre-existing inflammation, anatomical abnormalities, and excessive slope of the top of the tibia bone, which weaken the ligament. Rupture of the cruciate ligament in both knees is common. In fact, 54% of dogs will rupture the cranial cruciate ligament of the opposite stifle within a 3 year period of time.
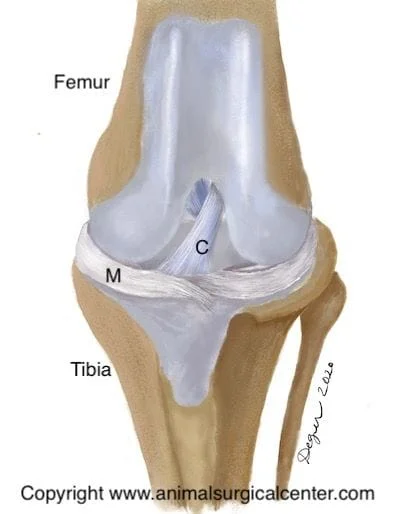
This front view of the canine stifle joint illustrates the cranial cruciate ligament (labeled C) and the medial meniscus (labeled M), which is a cartilage pad located within the stifle joint. This pad is commonly torn in dogs with cruciate ligament rupture.
Wagon Model Used to Explain Instability of the Knee Joint
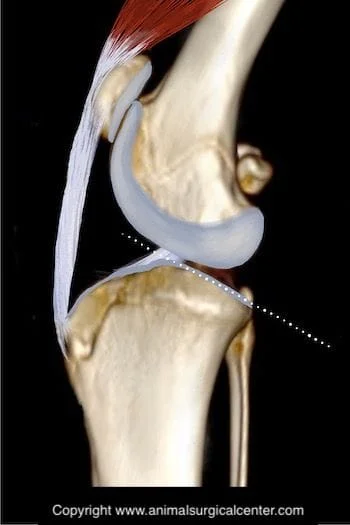
The tibial plateau of a dog’s stifle is sloped (see illustration left). Understanding the importance of the tibial slope when the cranial cruciate ligament is torn is somewhat difficult. We therefore present a model of a wagon on a hill, which is tied to a post with a rope. The slope of the hill represents the tibial plateau, the wagon represents the femur bone, and the rope represents the cranial cruciate ligament. If the rope is torn, the wagon will roll down the hill (see fig below). Likewise, when cranial cruciate ligament is torn the femur bone slides down the slope of the tibial plateau. When surface that the wagon is placed on is leveled and weight is put in the wagon, it does not to roll backward (see fig below). In the dog, the tibial plateau leveling osteotomy levels the slope of the tibial plateau so that the femur no longer slides down the plateau. Thus a dynamically stable joint is created even when no cruciate ligament is present.

Tibial Thrust
When the cruciate ligament is ruptured, the slope of the tibial plateau, along with the forces exerted by the calf and quadriceps muscles cause the femur bone to slide down the top of the tibia bone called the tibial plateau. This in essence causes the tibial plateau to thrust forward with each weight-bearing stride and is called cranial tibial thrust. This thrusting results in excessive wear of the cartilage of the joint. In addition, as the tibia thrusts forward it stretches the tissues which surround the joint, which causes pain. Excessive cranial tibial thrust also can tear of one of the cartilage pads in the knee called the medial meniscus. This usually results in a meniscal bucket handle tear or crush injury. The tibial plateau leveling osteotomy or TPLO can eliminate cranial tibial thrust, thus creating a dynamically stable stifle and sound gait.
Clinical signs
Clinical signs of early cruciate disease includes stiffness or very mild lameness. As the disease advances and the ligament progressively tears, the lameness becomes more pronounced. Some dogs show no lameness and then become profoundly lame after chasing a squirrel or other explosive activity. Complete tear of the ligament initially results in nonweight-bearing on the limb, but as time goes on the dog will assume a weight-bearing lameness. It is unusual that the lameness will resolve in a large breed dog without surgery.
Preparation for surgery
The pet should be fasted prior to surgery, as instructed by the surgical team. Water is usually permitted up to the time of admission to the hospital. The surgical team should be informed of any medications that your pet is currently receiving. Just prior to surgery, your pet will receive a sedative, have an intravenous catheter placed for the administration of intravenous fluids and intravenous medications, be induced under general anesthesia with medication(s), and have a breathing tube (endotracheal tube) placed to allow delivery of oxygen and gaseous anesthesia. The surgical site will be clipped and cleansed with an anti-septic solution in preparation for surgery. While under general anesthesia, the pet’s breathing will be assisted with a ventilator and vital parameters such as heart rate, respiratory rate, core body temperature, blood pressure, oxygenation of the blood (pulse oximetry), exhaled carbon dioxide (capnography), and heart rhythm (EKG) will be monitored to ensure the pet’s well being. Pain will be controlled both during and after surgery with analgesics (pain-controlling medication). Please note that each surgical and anesthesia team may elect to chose a different, but effective analgesia protocol.

TPLO Surgery
The first part of the surgery involves removing the torn ends of the cruciate ligament and examining the medial and lateral meniscus cartilages. To the right is an illustration of the front view of the stifle; note the medial meniscus has a dotted line draw on it which represents the typical location of a meniscal tear. The illustration below demonstrates a bucket handle tear of the medial meniscus (see arrow). This damaged portion of the meniscus or the entire medial meniscus is removed during surgery.

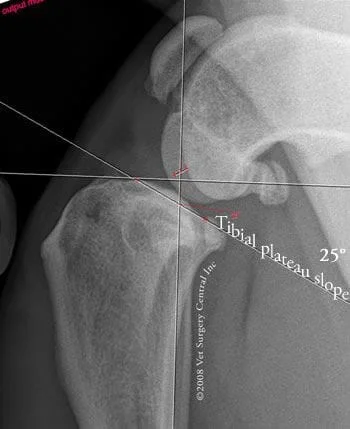
The tibial plateau leveling osteotomy involves making a curved cut in the top of the tibia bone (osteotomy) to include the tibial plateau. The tibial plateau is rotated along the curved osteotomy in order to level the slope. A plate and screws are used to hold the tibial plateau in place so that the bone can heal in its new position. Below left is an illustration of a stifle before TPLO surgery and below middle is an illustration demonstrating the curved cut in the tibia bone and rotation of the the tibial plateau. Take note in the illustration below right of the metal plate and screws that hold the bone together.



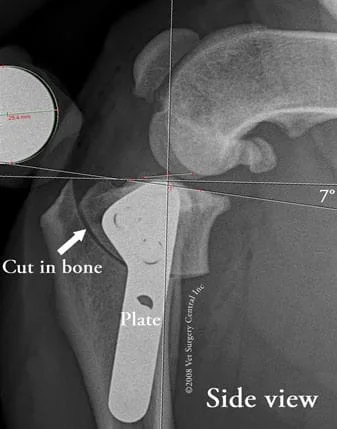

Take note of the radiograph on the right, which is a front view of the stifle after TPLO surgery. A plate is fastened in place with locking screws. It is critical to ensure that the screws do not penetrate through the top of the tibia bone into the stifle, as this will result in severe damage to the joint with resultant arthritis.
How to care for your pet after surgery
Surgery is only one part that will lead to a successful outcome. The second part is on the pet owner. Prescribed medications should be given to make sure that the pet's pain is well controlled, antibiotics to prevent infection and sedatives if the pet is hyperactive. Exercise must be restricted. Walking on the limb is not going to hurt the operated limb, but explosive activity is dangerous. Rehabilitation therapy is done at home and the recovery process may also be accelerated with the help of a rehabilitation therapist. Below is a video that demonstrates range of motion exercises that should be done after surgery. Your pet must not lick the incision, therefore an Elizabethan collar should be worn for the first 2 weeks after surgery.
Healing Phases Following TPLO surgery
Unlike the convalescence from other extra-articular or intra-articular techniques, recovery from TPLO surgery frequently is more rapid and complete. In our experience, about 50% of the dogs will start to walk on the limb within 24 hours after surgery. Within 5 days after surgery most dogs will bear weight on the operated limb. By 2 weeks after surgery, a moderate amount of weight-bearing can be expected. Dogs with partial tears tend to recover quicker than dogs having complete ligament tears. We have seen some dogs having partial tears recover to near full weight-bearing within 2 weeks after surgery…this is phenomenal, as we have never seen this type of a recovery with any of the other surgical techniques used to stabilize the stifle.
Radiographs taken at 8 weeks postop should reveal healing of the osteotomy site. At this time most dogs have mild to no lameness; when we evaluated our patients having TPLO, the average time for the lameness to resolve was 10 weeks. At 2 months after surgery, exercise in the form of leash walks should be gradually increased each week. Increasing the number of walks per day tends to be better than just increasing the duration of each period.
At 4 months after surgery most restrictions of exercise can be lifted. Full working activities (hunting, agility, etc) can begin at 5 months after surgery. Unconstrained activity prior to this time can cause spraining of the soft tissues of the stifle (patellar ligament sprain) resulting in a prolonged recovery. One study indicated a trend to a slower progression of arthritis following TPLO surgery, versus dogs that received the lateral imbrication technique, however arthritis usually will develop regardless of technique.
Success
One of the best things you can do to help your dog achieve a successful recovery is to follow the recommendations by a trained therapist. In addition, to learning what you can do at home, consider finding a canine rehabilitation facility in your area. A successful outcome will return your dog to full function on the limb. In my experience, about 90% of the dogs having the TPLO regain normal or near normal function of the limb (full weight-bearing); this information is based on a retrospective survey that we conducted on our patients. The remaining 10% of dogs have concurrent arthritis in other joints of the operated limb or advanced degenerative joint disease in the stifle; most of these dogs in this group are still helped by the surgery. We have found that most working dogs will return back to full working function. Dogs that have sustained a blowout fracture of the tibial plateau, as a complication of falling after surgery may have residual stiffness or lameness. Dogs that have been previously operated using another technique frequently respond well to the TPLO surgery. However, the best outcome is achieved in when only a TPLO surgery has been performed.
Potential complications
As with any surgery, complications may arise. Even though rare, anesthetic death can occur. With the use of modern anesthetic protocols and extensive monitoring devices (blood pressure, EKG, pulse oxymetry, inspiratory and expiratory carbon dioxide levels, and respiration rate), the risk of problems with anesthesia is minimized. Infection is an uncommon complication, as strict sterile technique is used during the surgery and antibiotics are administered during the procedure. We conducted a clinical study of the incidence of implant-associated infection at ASCM and found that in 800 consecutive cases, 1.9% of patients undergoing TPLO surgery eventually needed to have the metal implants removed due to infection. Elemental silver coated TPLO plates (HyProtect) will kill bacteria including those that are very resistant to antibiotics. No ill-effect of elemental silver-coated plates has been seen. Our impression is that use of this new generation of TPLO plate results in even fewer patients that develop infection after surgery.
Poor healing of the bone can occur if the pet is too active, especially during the first 2 months after surgery. If steroids are given to a pet for reasons such as skin allergies, healing of the bone may be severely impaired. Another study also demonstrated impaired bone healing when carprofen (Rimadyl) was administered to patients during the first 2 months after surgery. We have not seen retarded bone healing when a 10 day course of this medication has been administered after surgery.
After surgery, the soft tissues need to also heal and strengthen. If activity is unleashed prematurely, straining of the patellar ligament or other soft tissues can occur. Rest and anti-inflammatory medication is used to resolve this problem.
Fracture of the the tibial crest can occur. This is not common, and usually will heal without any surgical intervention. Recovery will be delayed, but the final result still should be good. In a clinical study that we conducted, we found that using preoperative measurements to guide the surgeon during surgery will help to maintain an ideally placed osteotomy and greatly reduced the risk of tibial crest fracture to 0% in this study.
A blow-out fracture of the tibial plateau has been seen in 0.4% of the cases (in a series of 700 cases) at our hospital. The cause of this was suspected to be due to the dog falling after surgery. Reoperation was performed in these cases. Since locking plates were adopted into standard practice of TPLO surgery, this complication has become rare.
Breakage of plates or screws or backing of screws out of the bone can occur if activity is not limited during the first 2 months. This is less common with locking plates and locking screws.
Loosening of the screws and subsequent shifting of the slope of the plateau may occur if the pet is not restricted during the healing phase. If the plateau has shifted a significant amount, reoperation may be needed. This complication is more common in the giant breed dog. As a result, two locking plates and screws may be used. It has been reported that dogs that have a very steep tibial slope (greater than 35 degrees) are at greater risk of having complications (shifting of the bones, fracturing of bones, loosening of implants). With the advent of locking TPLO plates and screws, this complication is greatly reduced.
A bone cancer can develop in the tibia bone due to the presence of the surgical implants (bone screws and plate); however, this complication is rare in our experience.
Arthritis usually is present at the time of surgery and will progress to some degree regardless of treatment or no treatment. Unfortunately, the arthritic and degenerative state of the joint cannot be reversed, but the surgery may help to slow the progression of this. I have seen cases receiving the TPLO surgery that have developed minimal arthritis years later, yet other cases have developed a significant degree of arthritis. Warning signs of clinical arthritis include stiffness associated with heavy exercise and cool damp weather. Anti-inflammatory medications can be useful to ameliorate a flare-up of arthritis.
Tearing of the meniscus (cartilage pad in the knee) may occur following TPLO surgery and meniscectomy will be needed to resolve the lameness.
