

Key Points
Osteosarcoma is the most common bone tumor in the dog
The traditional treatment for this problem is amputation which can be avoided with limb sparing surgery
Limb-spare surgery can be done in four different ways
Function of the limb following limb sparing is usually very good.
Limb sparing works best for osteosarcoma of the radius or ulnakey points
General Overview
- Osteosarcoma is the most common bone tumor in the dog.
- Other bone tumors such as chondrosarcoma and fibrosarcoma can affect the bone
- Over 10,000 new cases are reported each year in the United States.
- Any bone in either the limbs or spine or skull can be affected, with the lower part of the radius bone (bone of the front limb) being the most common location.
- Traditionally, surgical management for canine distal radial osteosarcoma has been amputation of the affected limb.
- Limb-spare surgery can be done for dogs that have cancer of the radius bone
- Reasons to avoid amputation and consider limb-sparing surgery instead
- concurrent degenerative joint disease (i.e. elbow dysplasia, hip dysplasia, cruciate rupture)
- neurologic disease
- size of dog being large – large and giant breeds
- Limb-spare surgery can be done in four different ways:
- Replacement of the radius bone with a bone from a cadaver (deceased dog)
- this technique is associated with a very high risk (about 50%) of chronic severe infection that cannot be cured with antibiotics
- this is the most common way that limb-spare surgery has been done
- this is the easiest way to do a limb-spare surgery
- this is NOT the best way to do a limb-spare surgery due to high infection rates
- Replacement of the radius by growing the bone using an Ilizarov technique
- in this technique the section of radius bone with the offending tumor is removed; a second cut is made near the end of the in the remaining stump of the radius bone (about 1 inch of bone); the small segment of bone is slowly moved at a rate of 1 mm per day down the region where the tumor was removed; as the bone segmented is slowly moved new bone forms, basically growing a new bone.
- this procedure can be very successful
- the main disadvantage to this technique is that it can take 4 to 6 months until the healing process is complete and a second surgery is needed to get the bottom portion of the traveling graft to unite with the wrist bones; during this time the dog must wear a circular external skeletal fixator, which is a set of rings and bars with pins that go through the skin a bones
- Replacement of the radius with a metal rod integrated in a plate construct
- the diseased section of radius is removed
- the implant is secured to the bones with screws
- this technique has shown some promising results
- implant is not commercially available to my knowledge, and is being used in clinical research
- Replacement of the radius by with a segment of the ulna bone (living graft) from the patient
- a segment of the ulna is harvested from the limb in which the tumor has been removed
- the blood supply to the ulnar bone graft is re-established using microsurgery; in some cases the ulna bone can be cut, leaving the blood supply intact, and “rolled” into the bony defect, thereby eliminating the need for microsurgery; a CT scan is usually needed to determine if your pet is a candidate for this technique
- this technique has a very low incidence of infection because the bone graft that is used to repair the limb is kept alive by re-establishing the blood supply to the graft
- the graft will rapidly heal to the bones and will become thicker in response to weight-bearing
- the final outcome generally is very good function of the limb
- this is the technique that I recommend due to the low complication rate
- the disadvantage of this technique is that the surgeon needs to be able to perform microsurgery and the procedure takes longer to perform than when a cadaver bone is used
- Replacement of the radius bone with a bone from a cadaver (deceased dog)
Criteria for a suitable candidate for vascularized limb-spare surgery
- The bone tumor is affecting the radius bone
- The tumor should be localized to the lower part of the bone
- No more than 1/3 of the bone should be affected
- The tumor should not have gross invasion into the soft tissues
- The patient should not have evidence of macroscopic metastatic disease (spread of cancer seen on chest radiographs)
- The patient should not have evidence of infection at tumor site
- The patient should not have any concurrent disease such as hyperadrenocorticism, which could make the patient hypercoagulable.
Staging and testing prior to surgery

- Complete blood cell count (CBC)
- Serum biochemistry profile
- Urinalysis
- Three view chest radiographs should be performed to rule out macroscopic pulmonary metastasis
- Radiographs of the affected limb are performed to determine cortical involvement of the radius and the adjacent ulna
- The use of computed tomography and magnetic resonance imaging may also help determine cortical and medullary involvement
- Whole body scintigraphy to check for spread of cancer to rest of body (ideal to do this prior to surgery)
- Tissue samples of the affected bone may be obtained for histopathology
- biopsies tracts should be carefully planned to avoid contaminating the adjacent distal ulna and surrounding soft tissue with cancer cells
- Heart ultrasound should be done to rule out cardiomyopathy as the adriamycin that may be used as a chemotherapeutic agent may cause heart failure if the heart is already in a weakened state
- Above right is an example of osteosarcoma tumor affecting the lower (distal) part of the radius bone in a Great Dane
Surgery
- The cancerous portion of the radius bone is removed

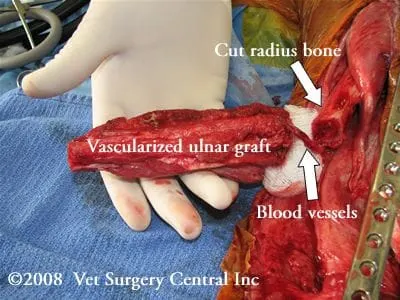
- A segment of the ulna bone on the same limb is harvested and placed in the defect
- The blood supply to the ulnar bone graft is reconnected using microsurgery (see photo right)
- A cancellous bone graft to help stimulate healing is harvested from the humerus bone (same limb as tumor)
- The cancellous bone graft from the humerus bone is packed into the wrist and around the ends of the ulnar graft
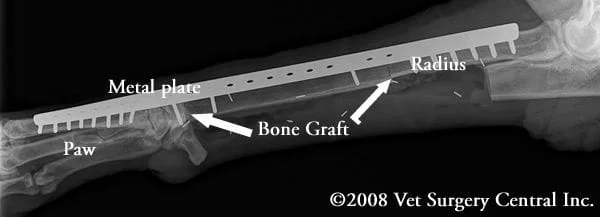
- A long plate and screws are used to hold the bones in place (in photo right the plate is fixed to the paw bones with screws)
- The resected radius bone is submitted for biopsy

- Below is a radiograph following surgery; the graft is held in place with two screws; a long plate and screws are the primary means of fixation
Postoperative management
- The limb is supported with a splint and bandage for 4 weeks
- Ultrasound doppler is performed during the first three days to make sure that the blood supply to the graft is still adequate
- Bone scintigraphy is performed within 7 days after surgery to ascertain ulnar graft viability
- Graft incorporation at the proximal and distal sites can be monitored via serial radiographs
- Viable grafts may show initial cortical bridging at four weeks, and complete incorporation at eight weeks
- Chemotherapy treatments should be started 2 weeks after surgery or once the skin incision has healed. Generally alternating doses of adriamycin and carboplatinum are administered every other week (3 doses of each drug).
- Chest radiography is performed every 3 months to monitor for metastasic disease.
Case examples
- Daphne, an 8-year-old Great dane developed osteosarcoma of the distal radius bone. She received a microvascular ulnar graft to reconstruct the right radius bone. Her gait is considered to be very good, but not perfectly normal. Her owner indicated that the dog can run and play with her other dogs. The video (right) demonstrates Daphne’s gait about 3 years after her initial surgery. She passed away about one month after this video was made as she developed another bone cancer in her hindlimb.
- Yukon, a 7-year-old yellow Labrador retriever developed osteosarcoma of the distal left radius bone. He received a limb sparing surgery using the ulnar roll-in technique. His gait is good, but not perfectly normal. He also had elbow dysplasia that likely was contributing to the gait abnormality. In general the function on the limb was considered to be very good. This video ( right) demonstrates Yukon’s gait after complete healing of the bone has taken place. Unfortunately, he died 7 months later due to cyclophosphamide toxicity.
- Hobo, a 9 year-old mixed breed dog, developed osteosarcoma of the left scapula (shoulder blade). He received a limb sparing surgery which involved removal of the top half of the scapula. He had a mild gait abnormality (lameness) that was persistent, but he had no recurrence of the local tumor and functioned much better than following amputation of the forelimb. The owner’s elected no chemotherapy after surgery. This video (right) demonstrates Hobo’s gait 2 months after surgery. Unfortunately he died 1 year after surgery due to metastatic disease, but he a had very good quality of life after surgery.
Potential complications
- Spread of cancer to lungs, bones or other areas on body
- Local recurrence of tumor – 10 to 20%
- Anesthetic death – rare
- Graft resorbtion
- Loosening of screws/implants
- Infection – may be cured with antibiotics
