

Key Points
The triple or double pelvic osteotomy is surgery used to treat hip dysplasia in immature dogs
Candidates for this surgery should:
- be less than 10 months of age
- have minimal to no arthritis
- have a crisp positive Ortolani sign
Lameness typically resolves in about 3 months after surgery
Success rate for this surgery is about 90%
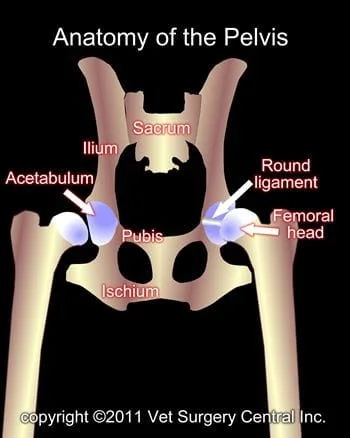
The pelvis is made of four bones: the ilium, acetabulum, pubis, and ischium. In the immature animal, these bones are not fused together, but as the pet matures, these bone fuse together in one confluent bone. The ilium joins the lower part of the spine called the sacrum.
The hip joint consists of a ball (femoral head) which is at the end of the femur bone and socket (acetabulum). This joint joins the hind limb to the pelvis. The joint is held together with a very strong round ligament (sometimes called the teres ligament) and the joint capsule. The muscles that surround the hip joint also provide very good support to the joint.
What is Hip dysplasia
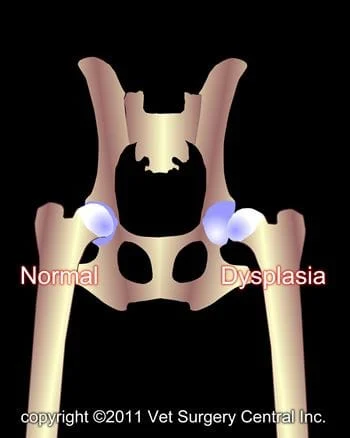
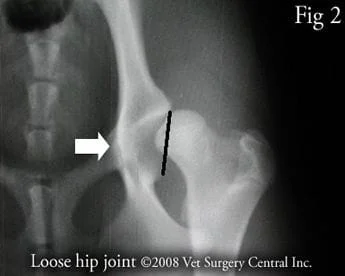
The first stage of hip dysplasia is looseness of the hip joints due to laxity of the ligament and joint capsule that holds the hip in place. In addition, pooly developed muscles of the hips can be a factor. Look at Fig 1 and 2 below and see the looseness of the left (L) hip joint (ball of femur not seated in socket) versus the right hip joint labeled R. One can be fooled by plain x-rays of the hips as they may appear to be fitting very well, but in reality they are quite loose. It is important to do a complete orthopedic examination to determine if the hip joint will pop in and out of the hip socket. If the joint is loose, the hip partially dislocates with each step the dog takes and the joint will gradually become deformed. The socket becomes shallow and the head of the femur becomes flattened. Arthritis develops in the joint and causes pain.
Occasionally, the hip joint will be very loose and it will become completely dislocated with minimal trauma. This usually causes the pet to become suddenly lame. Occasionally, only one hip has dysplasia, but more commonly both hips are affected.

Signs
Clinical signs of hip dysplasia can be seen as early as 4 months of age; however, many dogs are 5 to 8 months of age when a problem is first noticed. Early clinical signs of hip dysplasia start out as exercise intolerance (puppy only plays for short periods of time) or an awkward gait of the hind limbs. Bunny hopping, stiffness on rising after a rest, lameness, and atrophy of the muscles of the hind limbs are typical clinical signs. Some dogs seem to experience signs of hip dysplasia when they are a couple of years old and others in the geriatric years.
Diagnosis
A diagnosis of hip dysplasia is based on a combination of history, clinical signs, physical examination findings, and radiographs. A decision to perform a pelvic osteotomy should not be based only on radiographs. The ideal candidate for a pelvic osteotomy should have minimal to no degenerative osteoarthritis on radiographs and a positive Ortolani sign (the surgeon feel the hip crisply pop in and out of the joint during the examination). The angle at which the hip pops back in the joint should be less than 40 degrees (angle of reduction). In the event that your pet is not a candidate for a pelvic osteotomy, total hip replacement may be recommended.
Preparation for surgery
The pet should be fasted prior to surgery, as instructed by the surgical team. Water is usually permitted up to the time of admission to the hospital. An antacid such as Pepcid AC may be prescribed and should be administered by 6 AM on the day of surgery; this treatment will help reduce the risk of esophagitis (heartburn) in the postop period. The surgical team should be informed of any medications that your pet is currently receiving. The pet should not receive any aspirin within 1 week of surgery, as this medication will thin the blood and increase the risk of bleeding. Just prior to surgery, your pet will receive a sedative, have an intravenous catheter placed for the administration of intravenous fluids and intravenous medications, be induced under general anesthesia with medication(s), and have a breathing tube (endotracheal tube) placed to allow delivery of oxygen and gaseous anesthesia. The surgical site will be clipped and cleansed with an anti-septic solution in preparation for surgery. While under general anesthesia, the pet’s breathing will be assisted with a ventilator and vital parameters such as heart rate, respiratory rate, core body temperature, blood pressure, oxygenation of the blood (pulse oximetry), exhaled carbon dioxide (capnography), and heart rhythm (EKG) will be monitored to ensure the pet’s well being. Pain will be controlled both during and after surgery with analgesics (pain-controlling medication); we routinely place an epidural catheter for administration of narcotics during surgery and for two days after surgery. Please note that each surgical and anesthesia team may elect to chose a different, but effective analgesia protocol.
Pelvic osteotomy surgery
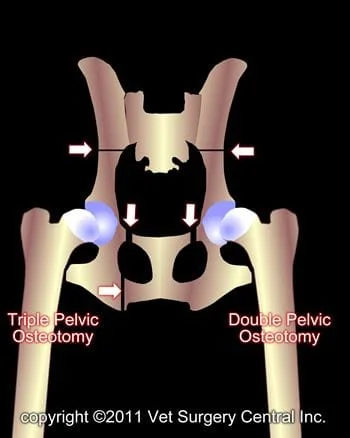
The TPO involves making three separate surgical incisions to cut the pelvis in three places (black lines denote cuts in the pelvis – fig below). One incision is in the groin, the second is on the rump, and the third is over the side of the hip region. The last incision is the largest of the three. The pelvis is cut in three places and then rotated to the desired amount. A plate and screws are used to secure the pelvis in the rotated position. The rotation of the pelvis captures the head of the femur, thus prevent the joint from popping in and out. Clinically this dog was pain-free and did not have any lameness after healing had taken place. Some arthritis has developed in the joint, but it usually does not progress to the degree of an unoperated dysplastic hip.
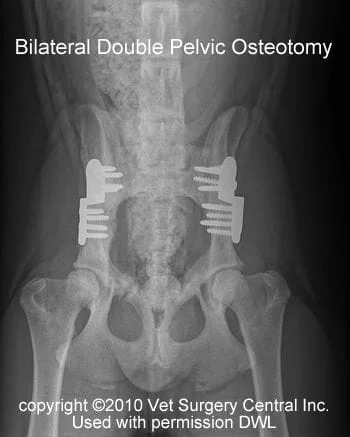
The double pelvic osteotomy (DPO) is preferred over the the triple pelvic osteotomy (TPO), as it results in less pain to the patient. With this procedure, only the ilium and the pubic bones are cut, leaving the ischium intact. Therefore, one less surgical incision is also needed. With the double pelvic osteotomy procedure, a specialized locking plate and locking screws are recommended. This also reduces the risk that the plate and screws will loosen in the postop period; x-ray right – months after surgery the femoral head is deeply seated in the cup of the hip joint. If the pelvis cannot be adequately rotated during the surgery will I resort to a TPO; this problem may be present if the patient is a little older (greater than 10 months of age).
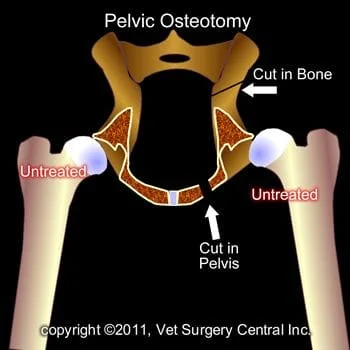
Before the pelvis has been rotated the femoral head does not seat very well in the acetabulum (labeled “Untreated”).
After the pelvis has been rotated, the femoral head is seated in the acetabulum (labeled “Treated”).
Below are illustrations that show how the TPO is done; take note of the rotation of the cut pelvic bone which then covers the head of the femur bone more effectively.


After care and convalescence
A prescribed oral pain reliever should be administered in the postop period at home. Nonsteroidal anti-inflammatory medications may be a part of the pain management protocol, but long-term administration of this medication is not recommended, as it may impede healing of the bone. In some cases, antibiotics may be prescribed.
A bandage may be applied to the incision until it is sealed. This bandage should be kept clean and only needs to be kept over the incision for about one or two days. The incisions should be checked daily for signs of infection during the first few weeks after surgery.
During the first 2 weeks after surgery, a sling should be placed under the belly, just in front of the hind limbs for the first 2 weeks to prevent slipping and falling when going outside. A bath towel or commercially available sling can be used for this purpose. Exercise restriction must be continued for 3 months. During the first 2 months the pet should be kept in the house on good footing (avoid slippery flooring); if needed put some throw rugs or strips of outdoor carpeting material on slippery floors. Short leash walks are permitted for elimination purposes. After the first 2 months, leash walks can be initiated and gradually increased.
The surgeon will monitor the healing process with at least two follow-up exams. The first is scheduled at two weeks after the surgery. During the second exam, at 6 weeks after the surgery, radiographs will be made again to evaluate the healing process.
By one day after surgery, most dogs will start to bear a mild to moderate amount of weight on the operated limb. By 6 to 8 weeks, the lameness should be dramatically improved. By 3 to 4 months after surgery, the pet should be completely sound on the operated limb(s).
Potential Complications
As with any surgery, complications may arise. Even though rare, anesthetic death can occur. Infection is also an unusual complication, as strict sterile technique is used during the surgery and antibiotics are administered during surgery. Excessive activity or exercise within the first 2 months can also lead to complications. The screws and plate that are used to hold the rotated pelvic bone in place could come loose or even break. This is not a concern once the bone has healed. The sciatic nerve which lies on the inner side of the pelvic bone could become bruised or damaged, which could result in loss of function of the limb. This is an unusual, but typically temporary complication. Obstruction of the urethra (tube leading from bladder) has been reported in the literature, but this is rare. Another complication could be severe progression of hip arthritis. In the event that this occurs and your pet has painful hip joints, a total hip replacement may be needed. Some arthritis will develop in the hip joint, but usually does not cause clinical lameness/stiffness. Development of severe arthritis that causes profound lameness is uncommon.
Prognosis
In general, about 90% of the dogs having the TPO or DPO surgery will be greatly improved, if not normal. Some mild arthritic changes can develop with time, but this usually does not cause signs of lameness or stiffness until the pet is geriatric.
Rev 9/15/11
